A wide variety of non-pharmacologic programs have been shown effective for controlling hospital acquired infections.
Infections are typically spread to and from hospital personnel, patients, and visitors.
Nosocomial infections kill between 90,000 and 100,000 patients per year.
Cost of each case infection has been estimated at between $15,000 and $25,000.
Handwashing remains the most effective way to reduce incidence of nosocomial infections.
Urinary-catheter associated infections remain the single most common type of nosocomial infection.
Transmission occurs by direct contact, via common vehicles (examination tables, instruments, etc.), and by airborne, droplet, and vector-borne mechanisms.
Recent data show that approximately 1.7 million infections occur in hospitals. Of these, about 1.3 million were contracted outside of the ICU. This works out to 9.3 infections per 1,000 patient-days or 4.5 per 100 admissions (1 out of 20 patients acquire an infection in U.S.). Nearly 100,000 deaths are attributable to nosocomial infections annually.
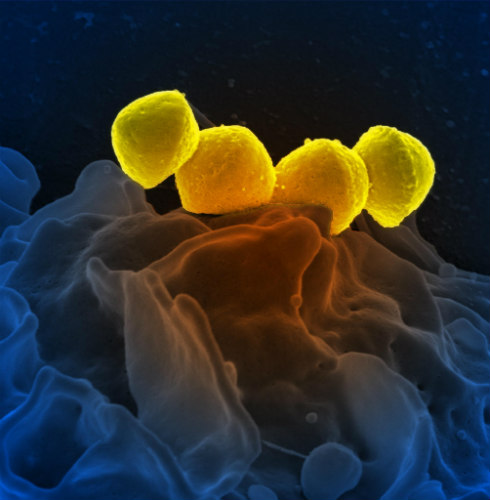
Figure 1. Group A Streptococcus bacteria on a human neutrophil.
Interventions are Cost Effective
Given the enormous personal and financial cost of these infections, numerous strategies have been attempted to limit the incidence of hospital acquired infections. A recent meta-analysis found cost savings of more than $13,000 per month per infection prevented.
Authors of the meta-analysis reviewed 27 studies that met the inclusion criteria. Overall, the review found nosocomial infection prevention programs to have significantly positive cost-benefit ratios. Interventions such as proper hand and surface cleaning, better nutrition, sufficient numbers of nurses, better ventilator management, use of coated urinary and central venous catheters, and the use of high-efficiency particulate air (HEPA) filters have all been associated with significantly lower nosocomial infection rates.
The simultaneous use of multiple strategies may offer the best opportunity to reduce the morbidity and mortality associated with hospital acquired infections. By reducing associated morbidity and mortality, these strategies will generally offer a return on investment by reducing or eliminating the the medical costs associated with these infections.
Effective non-pharmacologic interventions to prevent hospital acquired infections may also reduce the need for long courses or multiple-drug antibiotic courses for patients. Lower antibiotic drug usage will reduce risk of antibiotic-resistant organisms and should improve efficacy of antibiotics given to patients who do acquire infections, according to a report in the Journal of Hospital Infection.
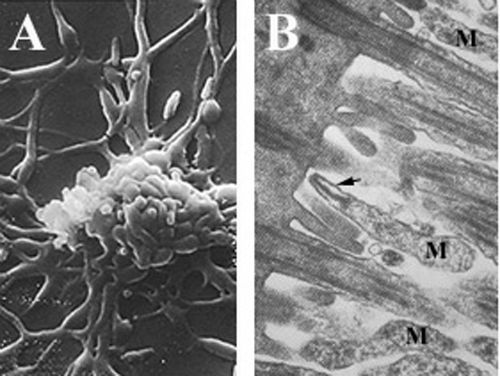
Figure 2.Mycoplasma pneumoniae on ciliated mucosal cells.
Interventions that Work
Isolation. Two types of isolation have been found effective:
Protective isolation for neutropenic or other immunocompromised patients to reduce the chances of acquiring opportunistic infections.
Source isolation of colonized or infected patients to minimize potential transmission to other patients or staff.
Identification of patients at risk. The following characteristic place patients at elevated risk of contracting a nosocomial infection:
Acute renal failure
Age ≥70 years
Coma
Drugs affecting the immune system (steroids, chemotherapy)
Indwelling catheters
Major trauma
Mechanical ventilation
Prior antibiotic exposure
ICU stay >3 days
Shock
Handwashing. Hands are the most common vehicle for transmission of organisms and handwashing is the single most effective means of preventing the transmission of infections among hospital patients and health care personnel.
Follow standard precautions. Conventional wisdom hold when it comes to preventing nosocomial infections. Proper usage of gloves, gowns, masks, and shoe and lace covers have been shown to be effective.
Patient-care equipment.
Used patient-care equipment soiled with blood, body fluids, secretions, or excretions should be handled carefully to prevent skin and mucous membrane exposures, contamination of clothing and transfer of microorganisms to HCWs, other patients or the environment.
Ensure that reusable equipment is not used for the care of another patient until it has been cleaned and sterilized appropriately.
Ensure that single use items and sharps are discarded properly.
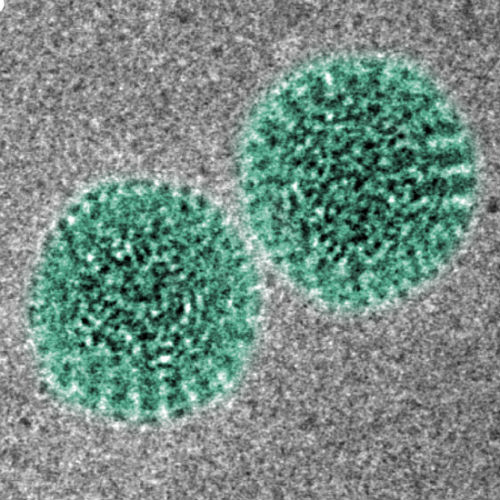
Figure 3. Rotavirus particles.
Follow Transmission-Based Precautions
In addition to standard precautions, the following should be observed in those patients known or suspected to have airborne, contact or droplet infections:
Airborne precautions:
Disease-causing microorganisms may be suspended in the air as small particles, aerosols, or dust and remain infective over time and distance. For example, Mycobacterium tuberculosis (pulmonary/laryngeal), varicella zoster virus (chickenpox), herpes zoster (shingles), rubella virus, and measles.
Isolate with negative-pressure ventilation.
Respiratory protection must be employed when entering the isolation room.
Use the disposable N-95 respirator mask, which fits tightly around the nose and mouth to protect against both large and small droplets. This should be worn by all persons entering the room, including visitors.
Contact precautions:
Infections can be spread by usual direct or indirect contact with an infected person, the surfaces or patient care items in the room, for example, parainfluenza virus infection, respiratory syncytial virus infection, varicella (chickenpox), herpes zoster, hepatitis A, and rotavirus infections.
Isolation is required.
Non-critical patient-care equipment should preferably be of single use. If unavoidable, then clean and disinfect them adequately before using to another patient.
Limit transport of the patient.
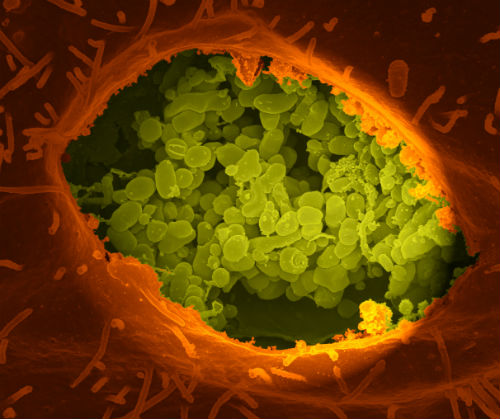
Figure 4.Coxiella burnetii. Droplet precautions:
Microorganisms are also transmitted by droplets (large particles >5 μm in size) generated during coughing, sneezing, and talking, or a short-distance traveling, for example, influenza virus, Bordetella pertussis, Hemophilus influenzae (meningitis, pneumonia), Neisseria meningitidis (meningitis, pneumonia, and bacteremia), Mycoplasma pneumoniae, Severe acute respiratory syndrome-associated coronavirus, Group A Streptococcus, adenovirus, and rhinovirus.
Isolation is required.
Respiratory protection must be employed when entering the isolation room or within 6-10ft of the patient. Use the disposable N-95 respirator mask, which fits tightly around the nose and mouth to protect against both large and small droplets. This should be worn by all persons entering the room, including visitors.